All surgery carries risks. The main risks are:
Bleeding and haematoma
Wounds can bleed after surgery. A build-up of blood under the skin is called a haematoma. A haematoma may require more surgery to remove it. A haematoma may affect the appearance of the end result.
Infection
A surgical wound can become infected. With surgery on uninfected clean skin this unlikely with less than 1 out of every 25 wounds becoming infected. These will usually settle with antibiotics but it is possible for the infection to form an abscess and then discharge through the wound or require surgery to drain it. Infection progressing to sepsis which is potentially life threatening is very rare in healthy people having skin surgery.
Wound breakdown and delayed healing
Wounds can open up or breakdown. This is most likely to happen if the wound is stressed in the early stages of healing or if it becomes infected. The wound will then usually heal ‘from the bottom up’ and this may take several weeks. The result is usually a wide scar that may be depressed. Some people may want further surgery to try and improve the appearance.
Poor scarring
Most people find the scar from surgery acceptable and worth the benefits of the surgery. The appearance of scar varies a lot from one person to another. Some people may very good nearly invisible scars when others with a similar wound may make an unsightly poor scar. Poorly planned surgery and complications like infection may well lead to poor scars. For other people a genetic tendency to make hypertrophic or keloid scars may result in a poor appearance of a scar. The section on the website about scarring has more details on poor scars.
Deformity after surgery
When a large lipoma is removed from under the skin it may result in a depression in the skin. The lipoma having pushed away the normal fat and tissues under the skin. Once the lipoma is removed there is an inevitable depression in the skin. These usually improve with time but to a degree are permanent.
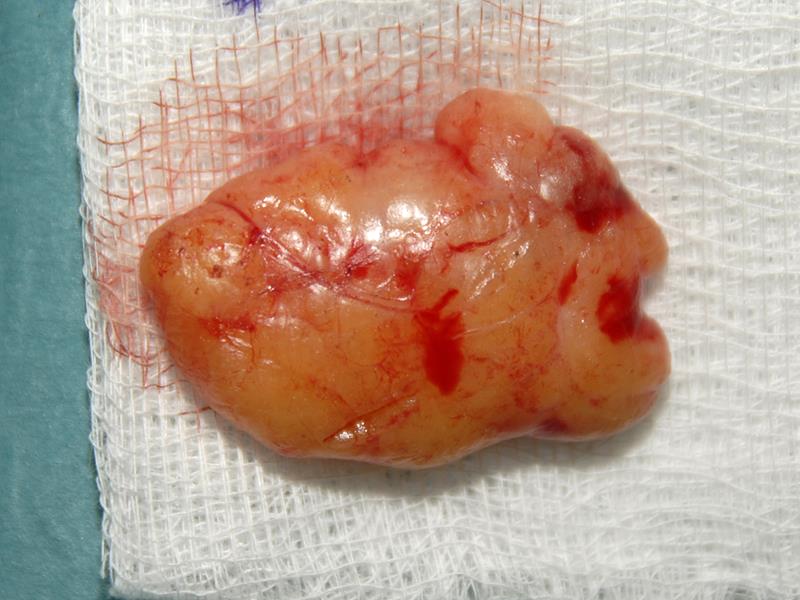
Recurrence of a lipoma
If a lipoma is completely removed it is unlikely to recur. If part of the lipoma is left behind when it is removed surgically then recurrence is much more likely.
If you have made one lipoma you are more likely to make more lipomas in the future.
Risks of not having a lipoma assessed or treated
There are risks of treatment but there are also risks of not having treatment. An untreated lipoma make enlarge and become more difficult to treat. A ‘lipoma’ that has not be assessed may turn out to be more serious than a simple lipoma.